

FDA + CMS Launch RAPID Coverage Pathway: A California Biomed Manager's Briefing
The FDA's device authorization programs and Medicare's coverage process have historically run on separate timelines, which meant a hospital could acquire a newly cleared or approved device months before a national or local coverage determination clarified how the procedure would be reimbursed. That gap has real operational consequences: capital committees hesitate, service contracts sit unsigned, and biomedical engineering inherits equipment before the supporting documentation and workflow are settled. The FDA and CMS have publicly discussed and piloted parallel-review and coordinated approaches precisely to shorten that lag for breakthrough and high-priority devices.
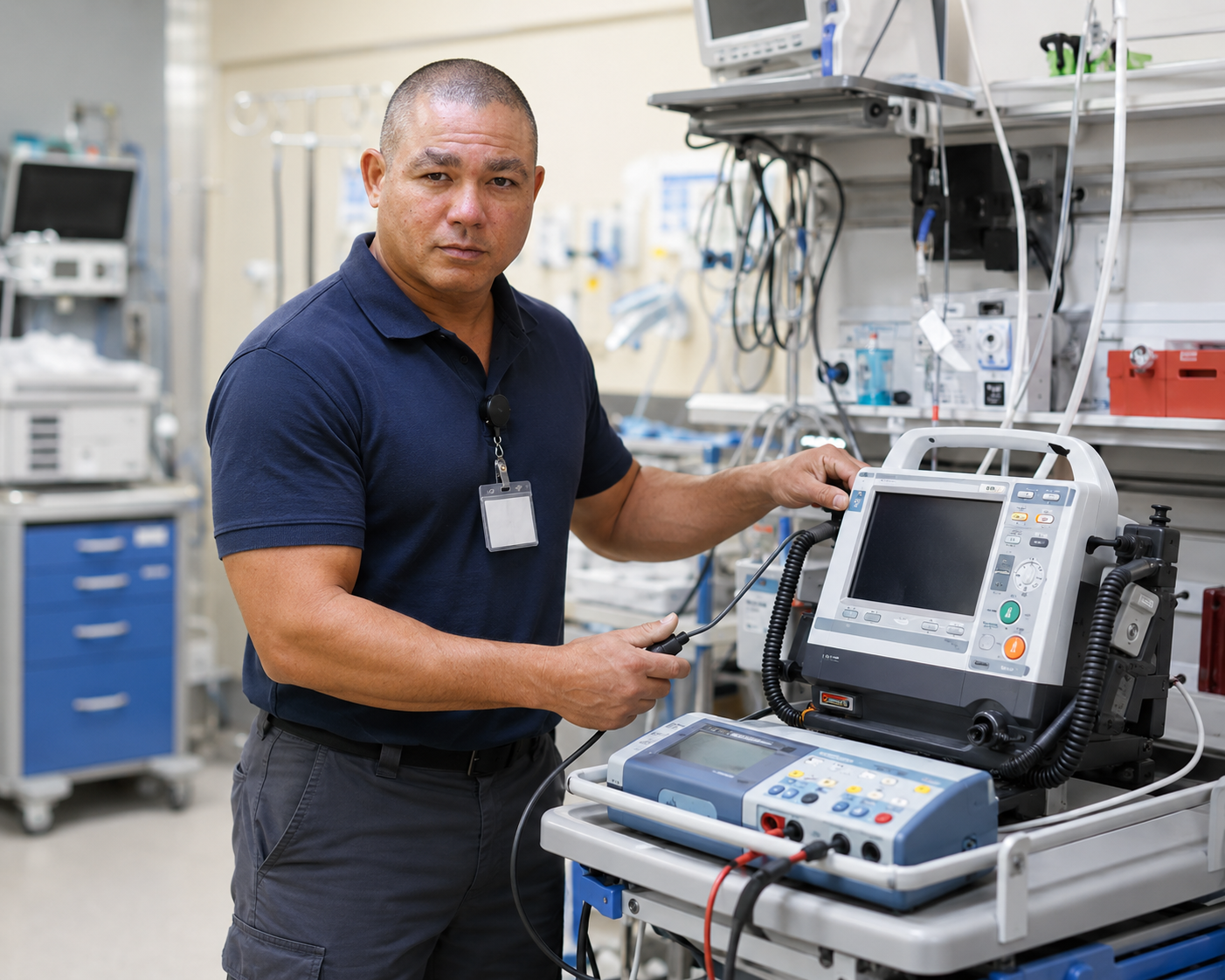
For California's academic medical centers and rural critical-access hospitals alike, any move toward parallel authorization and coverage changes the rhythm of new-equipment onboarding. Biomedical and healthcare technology management (HTM) teams should expect earlier service requests, tighter turnaround on incoming inspections, and a need to establish preventive maintenance intervals before a device is fully embedded in clinical workflow. Capital planning benefits from more predictable timelines, but only if HTM is looped in early rather than after purchase.
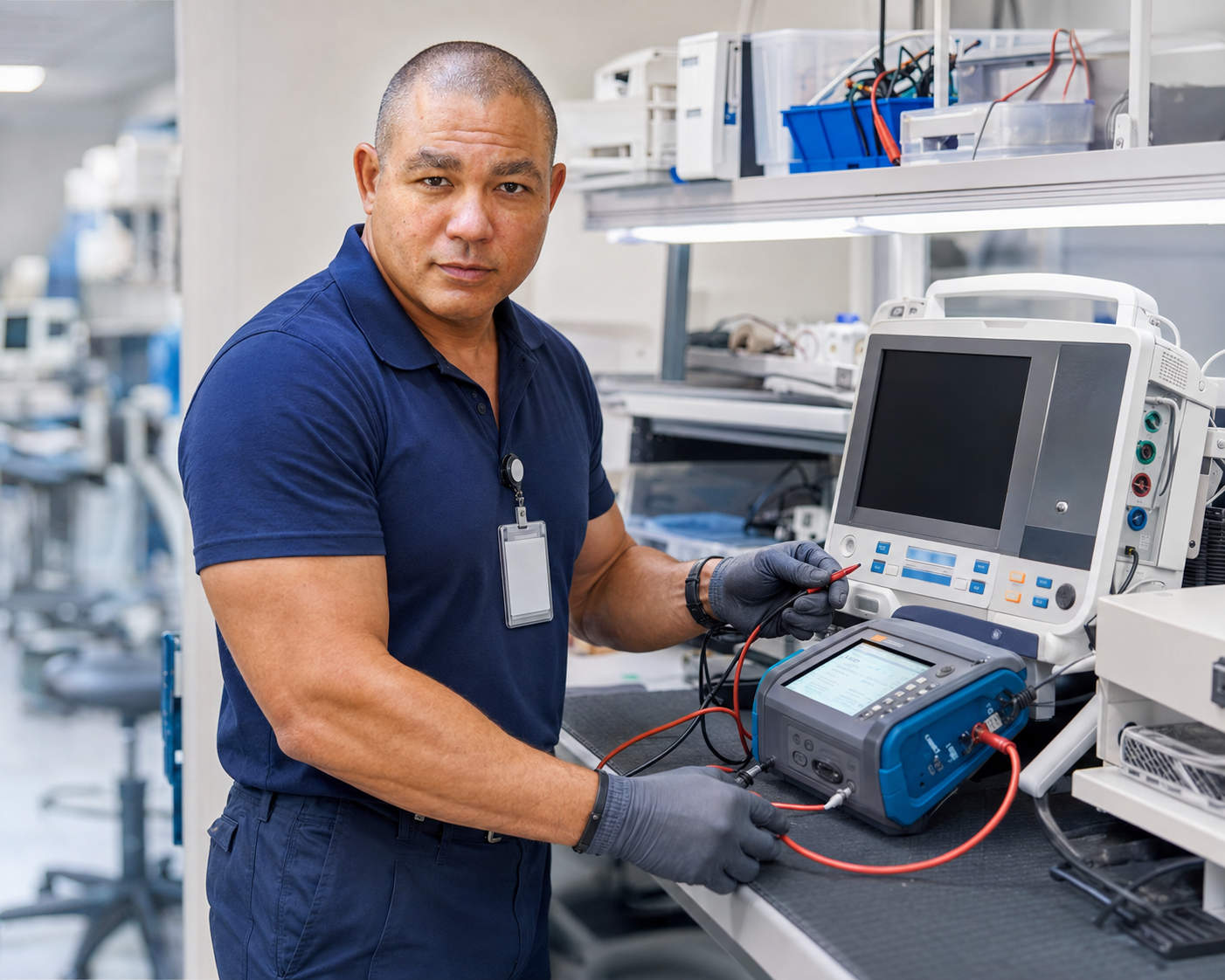
The practical takeaway for biomed managers is documentation discipline. Whatever the pathway, surveyors from The Joint Commission and CMS will still expect complete incoming-inspection records, calibration data, electrical safety testing, and a defined PM schedule tied to manufacturer recommendations and risk. Verify the current status and scope of any FDA and CMS coordinated pathway directly with the agencies before adjusting internal procedures, because program names and eligibility criteria evolve.
The specifics matter for planning capital purchases. CMS and the FDA announced the RAPID (Regulatory Alignment for Predictable and Immediate Device) coverage pathway on April 23, 2026, under which CMS can issue a proposed National Coverage Determination the same day the FDA authorizes an eligible Breakthrough Device — opening a 30-day comment window and enabling Medicare coverage as soon as roughly two months after clearance. Officials described about 40 devices as immediately qualifying, with another 20 potentially eligible, a large step up from the handful the earlier TCET pathway could handle each year. For a California hospital’s biomed department, faster coverage means new imaging and monitoring platforms can reach the floor sooner — and our calibration, preventive maintenance, and isolated-power testing keep them survey-ready from day one.
Sources: U.S. Food & Drug Administration; Centers for Medicare & Medicaid Services; The Joint Commission; FDA — CMS & FDA Announce RAPID Coverage Pathway